
Management of community-associated bacterial skin and soft tissue infections in children and prevention of recurrence
The Canadian Paediatric Society gives
permission to print single copies of this document from our website.
For permission to reprint or reproduce multiple copies, please see our copyright policy.
Principal author(s)
Justin Penner MD, Sergio Fanella MD; Canadian Paediatric Society,
Infectious Diseases and Immunization Committee
Abstract
Skin and soft tissue infections (SSTIs) are among
the most common infectious diseases encountered in children. Severity of
SSTIs range from simple infections that resolve spontaneously to severe
necrotizing syndromes requiring intravenous antibiotics, surgical
intervention, and intensive care. Inadequate skin barrier resulting from
common paediatric conditions such as eczema and skin abrasions
predisposes to infection. When antibiotics are needed, their choice and
duration should be guided by the most probable organisms involved, their
likely susceptibility profiles, and geographical epidemiologic
differences. Inappropriate treatment with overly broad-spectrum
antibiotics and/or for prolonged durations is detrimental to the
microbiomes of patients, increases antimicrobial-related side effects,
and perpetuates colonization of resistant organisms, precipitating
antimicrobial resistance. This statement provides health care providers
with a toolkit for optimal management of bacterial SSTIs, including
recurrent episodes. It does not comprehensively examine SSTI treatment
principles in immunocompromised or burn patients due to the management
complexities of both settings.
Keywords: Abscess; Cellulitis; Decolonization; MRSA; Skin infection
Background
The skin protects its host from infection by acting as a physical
barrier. Damage to this barrier from a variety of processes, including
atopic disease, skin irritants, xerosis, micro abrasions, ectoparasites
(e.g., scabies, lice), trauma, surgery, viral skin infections (e.g.,
herpes-zoster/herpes simplex [HZV/HSV]), or hair/nail infections,
increases vulnerability to infection.
Skin and soft tissue infections (SSTIs) are some of the most common
infectious diseases encountered in paediatrics. A Canadian multicentre
study of 12 remote/isolated communities estimated the prevalence of
SSTIs in some sites at 36.8%, with 60.2% of the total population studied
having received at least one antibiotic prescription in the preceding
12 months[1].
Such high antimicrobial use may be linked to higher rates of
antibiotic-resistant infections in these communities. Both the frequency
of SSTIs in the paediatric population and the potential for high
antimicrobial use resulting in infections with resistant organisms make
antimicrobial stewardship a public health issue of paramount concern.
This statement provides health care providers with a toolkit for
optimizing the management of bacterial SSTIs, including recurrent
episodes. It replaces previous guidance on methicillin-resistant Staphylococcus aureus (MRSA) skin abscesses from the Canadian Paediatric Society[2].
SSTIs have been categorized in various ways, without universal
consensus. A list of common terms can be found in Table 1. Bacterial
infections of the epidermis are typically less severe than deeper
infections, but they can facilitate bacterial entry into deeper tissues.
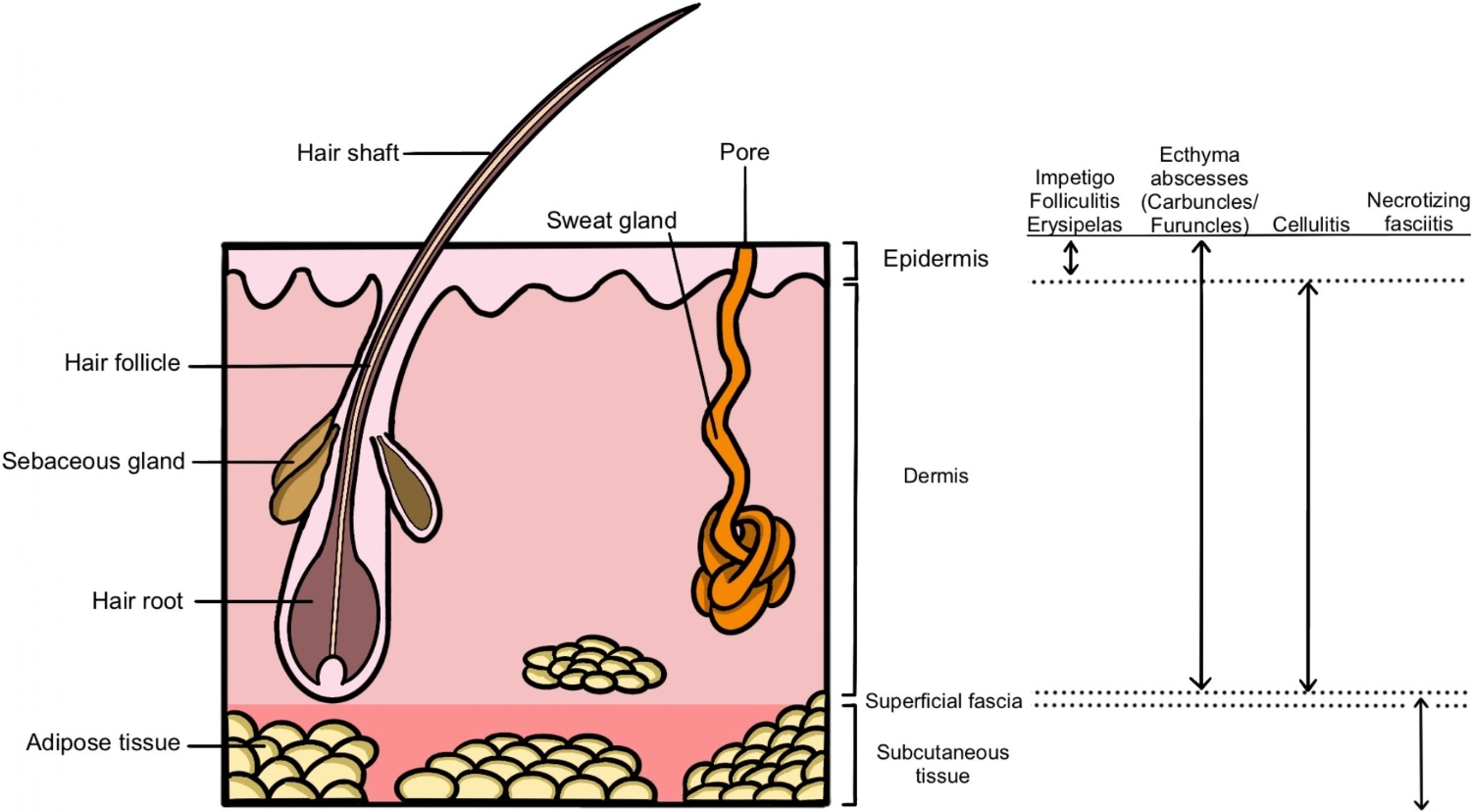
Abscesses can manifest in any of the tissue layers and are
characterized by discrete collections of pus (Figure 1).
Table 1. Skin and soft tissue infections: Terms and definitions*
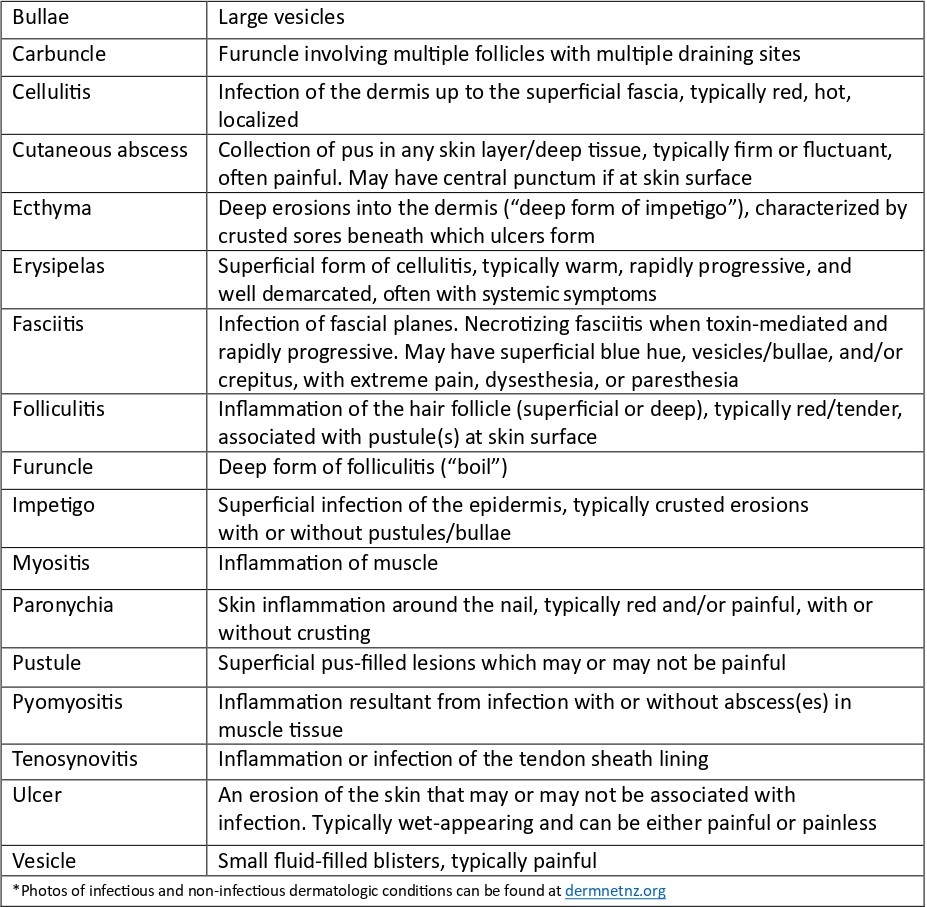
Figure 1. Skin and soft tissue infection anatomy
Delays in initiating treatment and inconsistencies in management
practices can cause disease progression, pain, deep-tissue abscesses,
musculoskeletal infections, and hypo- and hyperpigmentation.
Inappropriate antibiotic initiation, duration, and drug or route
selection for simple infections are detrimental to the individual’s
microbiome, increase antimicrobial-related side effects (e.g., Clostridioides difficile), and have societal impacts through increased antimicrobial resistance.
Microbiology
The most common pathogens associated with community-acquired bacterial SSTIs include methicillin-susceptible or -resistant Staphylococcus aureus (MSSA or MRSA) and Streptococcus pyogenes (Group A Streptococcus
[GAS]). Both pathogens can cause a range of SSTIs, from mild infections
(e.g., folliculitis, impetigo) to severe necrotizing infections
complicated by toxic shock or sepsis. Recent reports have suggested an
increase in invasive GAS infections[3]. Non-pyogenic cellulitis has been reported more with GAS compared with S. aureus, although microbiological confirmation is rare in this context and Canadian data is lacking in paediatric populations[4].
Although variable by province/territory, an increase in paediatric MRSA has been recognized in Canada[5][6].
This rise disproportionately impacts certain minoritized groups, such
as Indigenous communities in remote/isolated areas, where MRSA
proportions can exceed 50%[7]. Such prevalence indicates that certain social determinants of health, such as crowded housing, are risk factors for SSTIs[8]. Colonization rates of up to 67% have been reported in households where one member has had a recent MRSA infection[9]. Certain behaviours, such as nose-picking, have been associated with increasing rates of S. aureus carriage[10][11]. Some studies have shown that approximately one-third of individuals colonized with MRSA will develop an SSTI[12][13], and up to 70% with an MRSA SSTI may experience recurrence(s) over the following 6 to 12 months[14]. SSTI risk in children also increases with MSSA colonization[15].
Other bacterial pathogens and non-infectious mimics should be
considered based on exposure history and examination. Waterborne
pathogens include Aeromonas spp (in fresh water), Vibrio spp (in brackish or salt water), and Pseudomonas aeruginosa (causing
hot tub folliculitis, or ecthyma). Anaerobic bacteria can cause SSTIs
following a deep puncture wound or animal or human bite, and may feature
in cases of longstanding ulcerative lesions, immunocompromised hosts,
and prolonged or recent antimicrobial use. Consider non-tuberculous
mycobacteria, candida, moulds, and cutaneous dermatophytes when the
epidemiology or morphology of lesions suggests such etiologies. VZV
infections predispose to SSTIs, including invasive infections (e.g.,
necrotizing fasciitis)[16].
Eczema can also be superinfected with HSV (eczema herpeticum) or
enteroviruses (eczema coxsackium). Non-infectious mimics of SSTIs
include, but not limited to: pyoderma gangrenosum, pyogenic granuloma,
psoriasis, non-infected atopic dermatitis, hidradenitis suppurativa,
venous stasis or thrombosis, vasculitis, urticaria, contact dermatitis,
malignancy, and other non-infectious dermatologic or rheumatologic
conditions.
History and physical examination
The epidemiological triad comprises the host, pathogen, and
environment. A focused history should consider interactions among the
three, including preceding skin trauma, bites (animal or human), water
exposures, travel, sick contacts, social, occupational, and recreational
activities, and hospitalization(s) or frequent health care admissions
or attendance. Chronicity (i.e., acute, subacute, or chronic) and
associated symptoms (i.e., fever, pain) should form part of an SSTI
history. Past medical history should include personal and family
experience of previous SSTIs, underlying medical conditions, known
history or risk factors for MRSA colonization, and vaccination status.
While most children with recurrent SSTIs are immunocompetent, a careful
history should ensure there are no “red flags” for inborn errors of
immunity, such as recurrent, invasive, multi-site, or unusual
infections, early age of onset, deep skin or lymph node abscesses,
failure to thrive, and severe or intractable eczema. In cases of
recurrent perianal abscesses, inflammatory bowel disease should be
considered.
Severity assessments are largely subjective, though scoring systems
have been validated to help define mild, moderate, and severe disease.
One scoring system for cellulitis is the Melbourne ASSET score. Higher scores suggest increasing severity, with a cut-off of 4 limiting unnecessary intravenous (IV) antibiotics[17].
In a case-based survey of paediatricians, the most common findings
associated with severity and treatment with IV versus oral
antimicrobials included tracking lymphangitis, functional impairment of
the affected area, fever, oral antibiotics within the previous 24 hours,
size, site, and degree of swelling and tenderness[18].
Further findings suggestive of severe invasive disease include pain out
of proportion to clinical findings, rapidly expanding erythema,
necrosis, and crepitus.
Diagnostics
Microbiological samples should be sought for open wounds or lesions
with visible pus or fluid. Pus collected by needle aspirate, surgical,
or manual drainage of abscesses should be cultured and prioritized over
swabs based on their higher microbiological yield. Superficial swabs of
intact and non-intact skin or ulcers are of limited use due to isolation
of colonizing microbiota. If debridement is indicated, tissue samples
for culture are of highest yield. Other samples (e.g., skin biopsy) may
be considered in settings of chronic infection, failed therapy, an
immunocompromised child, or unusual exposure(s). In such cases, an
infectious disease (ID) or dermatology consult (or both) should be
sought to guide specimen requests. Specialized viral swabs from deroofed
vesicles placed in dedicated media are warranted for HSV, VZV, and
enterovirus polymerase chain reaction (PCR) testing. Blood cultures are
rarely indicated with clinically mild to moderate SSTIs but should be
collected with systemic illness, shock, and severe or deep-seated
infections. Dermatophyte and ectoparasite skin scrapings should be
collected when clinically indicated, following local laboratory
protocols.
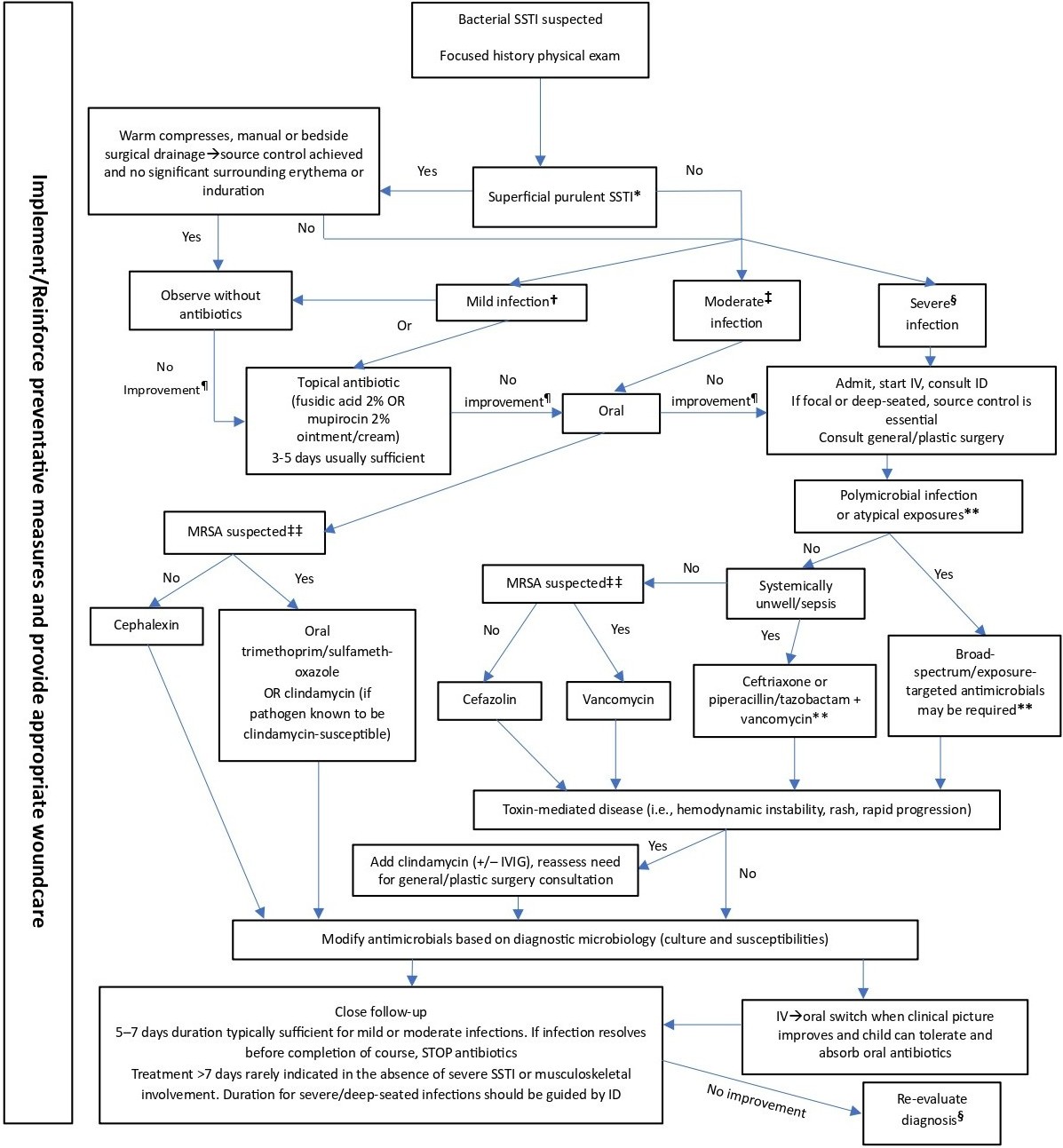
Management
(Figure 2)
Medical management
Clinicians should first consider whether antimicrobials are
warranted. Minor infections can resolve spontaneously with wound care
alone. Best practices for wound care management can be found at woundscanada.ca.
In addition to wound care, a short-course prescription (3 to 5 days) of
topical antimicrobials may be required. Evidence of benefit for
over-the-counter topical antimicrobials (e.g., polymyxin B, bacitracin,
neomycin) is unclear[19].
Empiric antimicrobial choices should be individualized based on history
(e.g., exposures), examination findings, and previous microbiology
results when available. More recent microbiological results should be
prioritized. Local paediatric-specific antibiograms are encouraged to
help guide empiric antimicrobial choice.
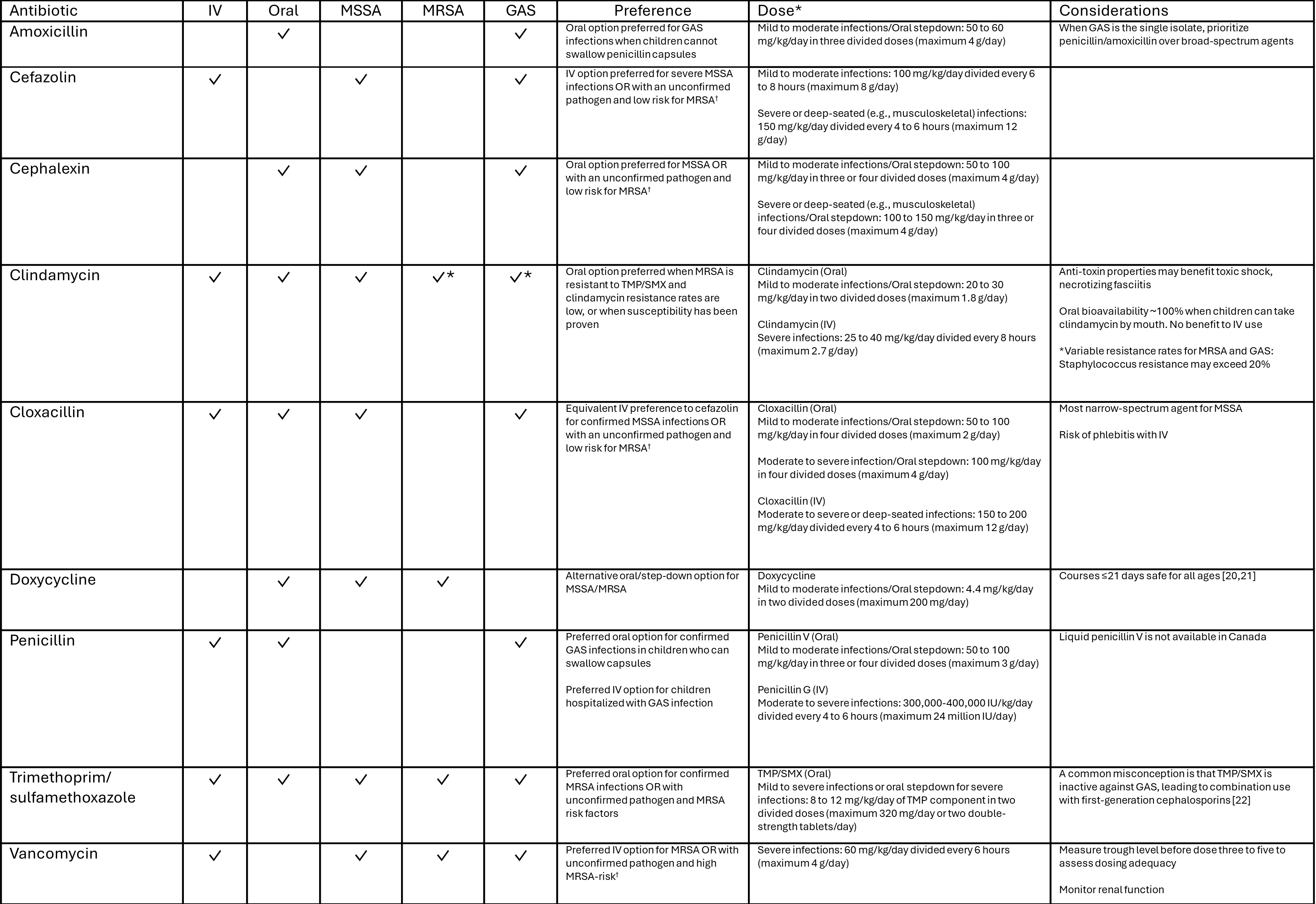
Empiric antibiotics should target the most common pathogens causing SSTIs (Table 2[20]-[22])
and most infections are amenable to oral treatment. In the majority of
cases, including moderate infections, oral cephalexin is appropriate,
provided that adequate dosing is administered[23].
Combination therapy with cephalexin and trimethoprim/sulfamethoxazole
or broad-spectrum outpatient IV antibiotics (e.g., ceftriaxone) are
discouraged. Empiric therapy targeting MRSA may be warranted in some
cases, such as when children are colonized or living in MRSA-prevalent
areas (i.e., where >10% to 15% S. aureus isolates are MRSA)[24].
Oral trimethoprim/sulfamethoxazole is preferred due to high
susceptibility rates for MRSA in Canada. Clindamycin resistance is
higher, although this antibiotic may still be considered for children
with prior susceptible isolates or when antibiograms demonstrate high
susceptibility. When a patient is known to be carrying MRSA (e.g.,
MRSA-positive nares) or later found to be after initiating
antimicrobials but has improved with non-MRSA treatment, switching
antimicrobials is not necessary. For children colonized with MRSA or
living in highly MRSA-endemic areas and presenting with a non-purulent
SSTI (e.g., cellulitis) without systemic features, consider initiating a
non-MRSA antimicrobial (e.g., cephalexin) with close follow-up[25][26].
For hospitalized children, antimicrobial choice is guided by the
history and severity of disease. For non-toxic children who have not
been exposed to atypical pathogens, IV cefazolin or, when MRSA is
suspected, vancomycin, is appropriate. For children who are systemically
unwell or toxic (e.g., concern for sepsis, fasciitis/myositis, shock),
many experts recommend initiating broad-spectrum coverage (ceftriaxone
or piperacillin-tazobactam, plus vancomycin) empirically, then
discontinuing vancomycin when MRSA is excluded. The addition of an
anti-toxin antibiotic (e.g., clindamycin) should be strongly considered
in such cases[27].
ID consultation should be sought and antibiotics targeted to
microbiology results. When SSTIs are complicated by a herpesvirus (e.g.,
HSV/VZV), IV acyclovir or oral acyclovir/valacyclovir may be warranted.
Table 2. Antimicrobials for treating systemic skin and soft tissue infections (SSTIs)
Surgical management
Source control of abscesses through surgical or manual drainage is
vital. Warm compresses can facilitate drainage. When drainage of an
uncomplicated small collection is achieved in a healthy host, without
significant surrounding cellulitis, antimicrobials are rarely warranted[28]-[30].
If antimicrobials were started previously, they can typically be
discontinued when drainage is achieved. Post-drainage wound care is
important for healing and consultation with experts in wound care may be
considered.
In cases of necrotizing infection, urgent surgical consultation for
debridement is essential. Deep samples of pus and tissue should be sent
for aerobic and anaerobic cultures. Debridement of chronic ulcers and
biopsies of unusual or chronic lesions and those failing therapy ensures
that tissue can be sent for bacterial, mycobacterial, and fungal
cultures and for histopathology to aid diagnosis and targeted therapy.
Figure 2. Treatment algorithm for skin and soft tissue infections (SSTIs)
Preventing recurrence
Preserving an intact skin barrier, including wound management and
control of primary dermatologic disorders, is important to prevent
SSTIs, including recurrence. Optimize eczema management, including
breaking the pruritus→scratch→skin breakdown cycle. Dermatology
consultation should be considered for children with difficult-to-control
skin conditions that threaten recurrence or serious infection.
In healthy patients, decolonization has achieved mixed results in
preventing SSTI recurrence, and treatment regimens and practices vary
with no clear consensus[31]-[36].
Decolonization practices can also be costly and dry the skin if
concurrent moisturizers are not used. Recurrence of colonization is
common, even with diligent decolonization practices[37]-[39].
Some experts reserve decolonization for recurrence of moderate to
severe SSTIs, household outbreaks, or to prepare for procedures with
high infection risk. Challenging cases often benefit from ID
consultation, and the advantages and disadvantages of treatments and
their variable success rates should be discussed with families. When
recommended, a 5-day trial of 2% mupirocin ointment twice daily to
nares, combined with daily cleaning with 4% chlorhexidine soap or 2%
chlorhexidine wipes (for 5 to 7 days) is suggested[40].
Dilute bleach baths (DBBs) are an acceptable alternative and can be
used as part of both decolonization regimens (daily for 5 to 7 days) or
maintenance suppression (or both)[41].
Concurrent family/household member decolonization may also be
considered to increase chances of decolonization success, although
evidence for this practice is inconsistent[42]-[44]. Use of oral antimicrobial agents for decolonization is discouraged unless directed by ID[31].
DBBs are prepared with 1/4 to 1/2 cup bleach added to a bathtub of
water. Children should be encouraged to sit in the bath for 5 to 10
minutes. Swimming in a chlorinated pool has similar effect. Maintenance
DBBs for children with a recurrent SSTI may be continued once or twice
per week to suppress bacterial microbiota. Make sure that skin
moisturizer is being applied after bathing. Concurrent environmental
decolonization measures in the household include cleaning surfaces with
bleach-containing solution, focusing on “high-touch” surfaces, washing
towels, clothing, and bedding in hot water, and replacing or
disinfecting personal hygiene items[45]-[47].
Sharing such items and sharing athletic equipment are discouraged. To
help maximize success, clinicians are encouraged to develop written
handouts describing these regimens, including images, detailed
instructions, with translation into local languages.
Additional measures to decrease recurrence include diligent wound
care, covering open wounds, encouraging universal uptake of varicella
vaccination, and regular cleaning of communal, sporting, and exercise
equipment (ideally after each use). Scabies and lice predispose to SSTIs
and should be treated per local guidelines[48][49].
Chronic antibiotic suppression is rarely indicated but may be
considered in consultation with ID for certain inborn errors of innate
immunity, chronic or recurrent dermatologic diseases, or conditions of
aberrant lymphatic drainage.
Recommendations
- Managing skin and soft tissue infections (SSTIs) should be based on
a focused history and careful assessment of the severity of infection.
- Empiric antimicrobial prescribing for SSTIs should be based on
locally sourced and paediatric-specific antibiograms. Prioritize the
most narrow-spectrum antimicrobial.
- Manage minor SSTIs with drainage and/or skin care alone. In select
cases, the addition of topical antimicrobial treatment may be required.
- Adequate drainage of abscesses negates the need to initiate
antimicrobials in most outpatient cases. If antimicrobials are
commenced, they can be discontinued when source control is achieved,
provided there is no significant surrounding cellulitis.
- When oral antimicrobials are warranted, cephalexin monotherapy is the antimicrobial of choice. When methicillin-resistant Staphylococcus aureus
is suspected, trimethoprim/sulfamethoxazole monotherapy is the
antimicrobial of choice for outpatient management. It also has activity
against Group A streptococcal infections.
- Short courses of antimicrobials (5 to 7 days) are often sufficient.
Longer treatment durations should be reserved for more severe or
complicated infections. Even severe SSTIs rarely require >7 days of
antimicrobials. Failure to respond should prompt re-evaluation of the
diagnosis and assessment for source control.
- Reserve intravenous antimicrobials for severe, deep-seated, or
necrotizing infections. Narrow-spectrum, short-courses of antimicrobials
should be prioritized based on microbiological testing, with a focus on
source control.
- Preventing recurrent SSTIs should focus on maintenance of intact
skin barrier, treatment of underlying skin conditions (e.g., eczema),
and good wound and abrasion care.
- In select individuals and households, decolonization protocols can be considered.
Acknowledgement
This position statement was reviewed by the Community Paediatrics and
First Nations, Inuit and Métis Health Committees of the Canadian
Paediatric Society (CPS). It was also reviewed by the CPS Community
Paediatrics, Hospital Paediatrics, and Paediatric Emergency Medicine
Section Executives, and by members of the Association of Medical
Microbiology and Infectious Disease Canada (AMMI).
CANADIAN PAEDIATRIC SOCIETY INFECTIOUS DISEASES AND IMMUNIZATION COMMITTEE (2024-2025)
Members: Michelle Barton MD (Chair), Laura Sauvé MD
(Past Chair), Eugene Ng MD (Board Representative), Ari Bitnun MD,
Jeannette Comeau MD MSc, Sergio Fanella MD, Justin Penner MD, MSc
Liaisons: Dorothy Moore MD (National Advisory Committee
on Immunization), Ari Bitnun MD (Canadian Paediatric and Perinatal
HIV/AIDS Research Group), Isabelle Viel-Thériault MD (Committee to
Advise on Tropical Medicine and Travel), Marina Salvadori MD (Public
Health Agency of Canada), Sean O’Leary (American Academy of Pediatrics,
Committee on Infectious Diseases), Rupeena Purewal MD (Immunization
Monitoring Program, ACTive), Cora Constantinescu MD (Association of
Medical Microbiology and Infectious Disease Canada, Pediatric Committee)
Principal authors: Justin Penner MD, Sergio Fanella MD
Funding
There is no funding to declare.
Potential Conflict of Interest
Dr. Fanella reported receiving funding as a local site PI for MCT for
COVID19 vaccines in children (ModernaTx). No other disclosures were
reported.
References
- Jeong D, Nguyen HNT, Tyndall M, Schreiber YS. Antibiotic
use among twelve Canadian First Nations communities: A retrospective
chart review of skin and soft tissue infections. BMC Infect Dis
2020;20(1):118. doi: 10.1186/s12879-020-4842-1
- Robinson JL, Salvadori MI; Canadian Paediatric Society,
Infectious Diseases and Immunization Committee. Management of
community-associated methicillin-resistant Staphylococcus aureus skin
abscesses in children. Paediatr Child Health 2011;16(2):115-6. doi:
10.1093/pch/16.2.115
- Centers for Disease Control and Prevention. Group A Strep Surveillance and Trends. July 8, 2024 (Accessed October 22, 2025).
- Stevens DL, Bryant AE. Impetigo, Erysipelas and
Cellulitis. February 10, 2016. In: Ferretti JJ, Stevens DL, Fischetti
VA, eds. Streptococcus pyogenes: Basic Biology to Clinical
Manifestations. Oklahoma City, OK: University of Oklahoma Health
Sciences Center; 2016.
- Nichol KA, Adam HJ, Golding GR, et al; Canadian
Antimicrobial Resistance Alliance (CARA) and CANWARD. Characterization
of MRSA in Canada from 2007 to 2016. J Antimicrob Chemother
2019;74(Suppl 4):iv55-iv63. doi: 10.1093/jac/dkz288
- Public Health Agency of Canada. Canadian Antimicrobial Resistance Surveillance System (CARSS) Report 2022. January 2023 (Accessed October 22, 2025).
- Fanella S, Embree J. Pediatric Staphylococcus aureus
infections: Impact of methicillin resistance at a Canadian center. South
Med J 2015;108(5):254-7. doi: 10.14423/SMJ.0000000000000274
- Butler-Jones D, Wong T. Infectious disease, social
determinants and the need for intersectoral action. Can Commun Dis Rep
2016;42(Suppl 1):S118-S120.
- Fritz SA, Hogan PG, Hayek G, et al. Staphylococcus
aureus colonization in children with community-associated Staphylococcus
aureus skin infections and their household contacts. Arch Pediatr
Adolesc Med 2012;166(6):551-7. doi: 10.1001/archpediatrics.2011.900
- Loewen K, Schreiber Y, Kirlew M, Bocking N, Kelly L.
Community-associated methicillin-resistant Staphylococcus aureus
infection: Literature review and clinical update. Can Fam Physician
2017;63(7):512-20. Erratum in: Can Fam Physician 2017;63(8):596.
- Wertheim HFL, van Kleef M, Vos MC, Ott A, Verbrugh HA,
Fokkens W. Nose picking and nasal carriage of Staphylococcus aureus.
Infect Control Hosp Epidemiol 2006;27(8):863-7. doi: 10.1086/506401
- Ellis MW, Hospenthal DR, Dooley DP, Gray PJ, Murray CK.
Natural history of community-acquired methicillin-resistant
Staphylococcus aureus colonization and infection in soldiers. Clin
Infect Dis 2004;39(7):971-9. doi: 10.1086/423965
- Yang ES, Tan J, Eells S, Rieg G, Tagudar G, Miller LG.
Body site colonization in patients with community-associated
methicillin-resistant Staphylococcus aureus and other types of S. aureus
skin infections. Clin Microbiol Infect 2010;16(5):425-31. doi:
10.1111/j.1469-0691.2009.02836.x
- Creech CB, Al-Zubeidi DN, Fritz SA. Prevention of
recurrent staphylococcal skin infections. Infect Dis Clin North Am
2015;29(3):429-64. doi: 10.1016/j.idc.2015.05.007
- Faden H, Lesse AJ, Trask J, et al. Importance of
colonization site in the current epidemic of staphylococcal skin
abscesses. Pediatrics 2010;125(3):e618-24. doi: 10.1542/peds.2009-1523
- Davies HD, McGeer A, Schwartz B, et al. Invasive group A
streptococcal infections in Ontario, Canada. Ontario Group A
Streptococcal Study Group. N Engl J Med 1996;335(8):547-54. doi:
10.1056/NEJM199608223350803
- Ibrahim LF, Hopper SM, Donath S, Salvin B, Babl FE,
Bryant PA. Development and validation of a cellulitis risk score: The
Melbourne ASSET Score. Pediatrics 2019;143(2):e20181420. doi:
10.1542/peds.2018-1420
- Ibrahim LF, Babl FE, Hopper SM, Bryant PA. Cellulitis:
Oral versus intravenous and home versus hospital—What makes clinicians
decide? Arch Dis Child 2020;105(4):413-15. doi:
10.1136/archdischild-2019-316824
- Banerjee S, Argáez C. Topical antibiotics for infection
prevention: A review of the clinical effectiveness and guidelines.
Ottawa, Ont.: Canadian Agency for Drugs and Technologies in Health;
March 30, 2017.
- Kimberlin DW, Banerjee R, Barnett ED, Lynfield R, Sawyer
MH. Tetracyclines. In: Red Book: 2024–2027 Report of the Committee on
Infectious Diseases (33rd edn.). Itaska, IL: American Academy of
Pediatrics; May 2024.
- Ravindra D, Huang G, Hallett K, Burgner DP, Gwee A,
Silva MJ. Antibiotic exposure and dental health: A systematic review.
Pediatrics 2023;152(1):2023061350. doi: 10.1542/peds.2023-061350
- McCreary EK, Johnson MD, Jones TM, et al. Antibiotic
myths for the infectious diseases clinician. Clin Infect Dis
2023;77(8):1120-5. doi: 10.1093/cid/ciad357. Erratum in: Clin Infect Dis
2024;78(6):1780.
- Trottier ED, Farley St-Amand B, Vincent M, et al.
Outpatient management of moderate cellulitis in children using high-dose
oral cephalexin. Paediatr Child Health 2022;27(4):213-9. doi:
10.1093/pch/pxac031
- Kaplan SL. Treatment of community-associated
methicillin-resistant Staphylococcus aureus infections. Pediatr Infect
Dis J 2005;24(5):457-8. doi: 10.1097/01.inf.0000164162.00163.9d
- Eells SJ, Chira S, David CG, Craft N, Miller LG.
Non-suppurative cellulitis: Risk factors and its association with
Staphylococcus aureus colonization in an area of endemic
community-associated methicillin-resistant S. aureus infections.
Epidemiol Infect 2011;139(4):606-12. doi: 10.1017/S0950268810001408
- Rajan S. Skin and soft-tissue infections: Classifying
and treating a spectrum. Cleve Clin J Med 2012;79(1):57-66. doi:
10.3949/ccjm.79a.11044
- Farrell CA. Diagnosis and management of severe sepsis in
the paediatric patient. Paediatr Child Health 2020;25(7):475-6. doi:
10.1093/pch/pxz178
- Singer AJ, Thode HC. Systemic antibiotics after incision
and drainage of simple abscesses: A meta-analysis. Emerg Med J
2014;31(7):576–8. doi: 10.1136/emermed-2013-202571
- Daum RS, Miller LG, Immergluck L, et al. A
placebo-controlled trial of antibiotics for smaller skin abscesses. N
Engl J Med 2017;376(26):2545–55. doi: 10.1056/NEJMoa1607033
- Wang W, Chen W, Liu Y, et al. Antibiotics for
uncomplicated skin abscesses: Systematic review and network
meta-analysis. BMJ Open 2018;8(2):e020991. doi:
10.1136/bmjopen-2017-020991
- Helbo T, Boel JB, Bartels MD, Ahlström MG, Holzknecht
BJ, Eriksen HB. Carriage of methicillin-resistant Staphylococcus aureus
in children <6 years old: A retrospective follow-up study of the
natural course and effectiveness of decolonization treatment. J
Antimicrob Chemother 2024;79(4):826-34. doi: 10.1093/jac/dkae036
- Piewngam P, Otto M. Staphylococcus aureus colonisation
and strategies for decolonisation. Lancet Microbe 2024;5(6):e606-18.
doi: 10.1016/S2666-5247(24)00040-5
- Klempner MS, Styrt B. Prevention of recurrent
staphylococcal skin infections with low-dose oral clindamycin therapy.
JAMA 1988;260(18):2682-5.
- Raz R, Miron D, Colodner R, Staler Z, Samara Z, Keness
Y. A 1-year trial of nasal mupirocin in the prevention of recurrent
staphylococcal nasal colonization and skin infection. Arch Intern Med
1996;156(10):1109-12.
- Coates T, Bax R, Coates A. Nasal decolonization of
Staphylococcus aureus with mupirocin: Strengths, weaknesses and future
prospects. J Antimicrob Chemother 2009;64(1):9-15. doi:
10.1093/jac/dkp159
- Creech CB, Beekmann SE, Chen Y, Polgreen PM. Variability
among pediatric infectious diseases specialists in the treatment and
prevention of methicillin-resistant Staphylococcus aureus skin and soft
tissue infections. Pediatr Infect Dis J 2008;27(3):270-2. doi:
10.1097/INF.0b013e31815c9068
- Doebbeling BN, Reagan DR, Pfaller MA, Houston AK, Hollis
RJ, Wenzel RP. Long-term efficacy of intranasal mupirocin ointment. A
prospective cohort study of Staphylococcus aureus carriage. Arch Intern
Med 1994;154(13):1505-8. doi: 10.1001/archinte.1994.00420130101013
- Fernandez C, Gaspar C, Vindel AT, Saez-Nieto JA, Cruzet
F, Aguilar L. A double-blind, randomized, placebo-controlled clinical
trial to evaluate the safety and efficacy of mupirocin calcium ointment
for eliminating nasal carriage of Staphylococcus aureus among hospital
personnel. J Antimicrob Chemother 1995;35(3):399-408. doi:
10.1093/jac/35.3.399
- Mody L, Kauffman CA, McNeil SA, Galecki AT, Bradley SF.
Mupirocin-based decolonization of Staphylococcus aureus carriers in
residents of 2 long-term care facilities: A randomized, double-blind,
placebo-controlled trial. Clin Infect Dis 2003;37(11):1467-74. doi:
10.1086/379325
- Whitman TJ, Herlihy RK, Schlett CD, et al.
Chlorhexidine-impregnated cloths to prevent skin and soft-tissue
infection in Marine recruits: A cluster-randomized, double-blind,
controlled effectiveness trial. Infect Control Hosp Epidemiol
2010;31(12):1207-15. doi: 10.1086/657136
- Fisher RG, Chain RL, Hair PS, Cunnion KM. Hypochlorite
killing of community-associated methicillin-resistant Staphylococcus
aureus. Pediatr Infect Dis J 2008;27(10):934-5. doi:
10.1097/INF.0b013e318175d871
- Fritz SA, Hogan PG, Hayek G, et al. Household versus
individual approaches to eradication of community-associated
Staphylococcus aureus in children: A randomized trial. Clin Infect Dis
2012;54(6):743-51. doi: 10.1093/cid/cir919
- Wiese-Posselt M, Heuck D, Draeger A, et al. Successful
termination of a furunculosis outbreak due to lukS-lukF-positive,
methicillin-susceptible Staphylococcus aureus in a German village by
stringent decolonization, 2002-2005. Clin Infect Dis 2007;44(11):e88-95.
doi: 10.1086/517503
- Hogan PG, Parrish KL, Mork RL, et al. HOME2 Study: Household versus
personalized decolonization in households of children with
methicillin-resistant Staphylococcus aureus skin and soft tissue
infection—A randomized clinical trial. Clin Infect Dis
2021;73(11):e4568-77. doi: 10.1093/cid/ciaa752
- Hogan PG, Mork RL, Thompson RM, et al. Environmental
methicillin-resistant Staphylococcus aureus contamination, persistent
colonization, and subsequent skin and soft tissue infection. JAMA
Pediatr 2020;174(6):552-62. doi: 10.1001/jamapediatrics.2020.0132
- Huang SS, Singh R, McKinnell JA, et al; Project CLEAR
Trial. Decolonization to reduce postdischarge infection risk among MRSA
carriers. N Engl J Med 2019;380(7):638-50. doi: 10.1056/NEJMoa1716771
- Mork RL, Hogan PG, Muenks CE, et al. Longitudinal,
strain-specific Staphylococcus aureus introduction and transmission
events in households of children with community-associated
meticillin-resistant S aureus skin and soft tissue infection: A
prospective cohort study. Lancet Infect Dis 2020;20(2):188-98. doi:
10.1016/S1473-3099(19)30570-5
- Banerji A; Canadian Paediatric Society, First Nations,
Inuit and Métis Health Committee. Scabies. Paediatr Child Health
2015;20(7):395-402. doi: 10.1093/pch/20.7.395
- Cummings C, Finlay JC, MacDonald NE. Head lice
infestations: A clinical update. Paediatr Child Health
2018;23(1):e18-e24. doi: 10.1093/pch/pxx165
Disclaimer: The
recommendations in this position statement do not indicate an exclusive
course of treatment or procedure to be followed. Variations, taking into
account individual circumstances, may be appropriate. Internet
addresses are current at time of publication.









{kind=link}