Ένα
στα τρία παιδιά σε όλη την Ευρώπη υποφέρει σήμερα από κάποιας μορφής
αλλεργία –έτσι οι γονείς πρέπει να είναι πολύ προσεκτικοί στην
παρακολούθηση και τον εντοπισμό των συμπτωμάτων. Τι πρέπει να γνωρίζουν,
λοιπόν, τόσο για την ασθένεια όσο και για τη θεραπεία;
Ορισμός
Κληρονομική ευαισθησία που εκδηλώνεται σαν έντονη οξεία η χρόνια αντίδραση σε κάτι μη παθολογικό.
Γιατί συμβαίνει
Διότι
το ανοσοποιητικό σύστημα αντιδρά υπερβολικά σε μια «αθώα» ουσία, όπως
γάλα, σκόνη, μέλισσα (αλλεργιογόνα) που την θεωρεί «εχθρό».
Συνήθως με συμπτώματα από το δέρμα, αναπνευστικό, γαστρεντερικό.
Οξέα αλλεργικά νοσήματα
Κνίδωση εμφανίζεται με κοκκινίλα στο σώμα, άκρα η πρόσωπο. Αγγειοοίδημα,Αναφυλαξία, η Αλλεργικό σοκ
είναι σοβαρές οξείες αντιδράσεις. Εκδηλώνονται με απότομο πρήξιμο στο
πρόσωπο, στα χείλη, τα μάτια, αυτιά, η αλλού στο σώμα, με η χωρίς
εξάνθημα. Αν παρουσιαστεί βραχνάδα, δυσκολία αναπνοής, πόνος στην κοιλιά
η ζαλάδα η κατάσταση είναι πολύ σοβαρή και πρέπει να αντιμετωπιστεί
άμεσα στα επείγοντα.
Χρόνια αλλεργικά νοσήματα. Ρινίτιδα, Επιπεφυκίτιδα, Βρογχίτιδα/ Άσθμα, Έκζεμα, εξανθήματα.
Πως εκδηλώνονται
Ρινίτιδα: μύτη που συχνά τρέχει, «γαργαλάει» ή μπουκώνει. Συχνά οι εκκρίσεις από τη μύτη κατεβαίνουν στον λαιμό και προκαλούν βήχα.
Επιπεφυκίτιδα: φαγούρα και κόκκινα μάτια.
Άσθμα:
συχνές ιώσεις, βρογχίτιδες η λαρυγγίτιδες. Συχνός βήχας η συριγμός
(σφύριγμα) ανεξάρτητα από κρυολόγημα, βήχας στην άσκηση, εύκολο
λαχάνιασμα, δυσκολία αναπνοής ή δύσπνοια, σφίξιμο στο στήθος.
Έκζεμα: ξηρό δέρμα με φαγούρα που συχνά μολύνεται με σταφυλόκοκκο.
Η διάγνωση
της αλλεργίας για εντοπισμό του ένοχου αλλεργιογόνου βασίζεται στο
ιστορικό αλλά και στις εξετάσεις αίματος ή δερματικές. Όμως, πρέπει
πάντα να συσχετίζονται τα συμπτώματα του παιδιού με τις εξετάσεις γιατί
αυτές μπορεί να είναι ψευδώς θετικές.
Η θεραπεία των αλλεργιών στοχεύει στην εξάλειψη των συμπτωμάτων και ανάλογα με την περίπτωση, περιλαμβάνει:
Την απομάκρυνση/ αποφυγή από το ένοχο αλλεργιογόνο.
Την θεραπεία με αντιισταμινικά φάρμακα ή/και εισπνεόμενα για τη μύτη ή τους πνεύμονες ή κορτιζόνη.
Απευαισθητοποίηση
στο αλλεργιογόνο, σε χρόνια αλλεργία, αν με τα φάρμακα δεν βελτιώνεται
το παιδί και δεν είναι δυνατή η απομάκρυνση του αλλεργιογόνου.
Εφοδιασμό με ένεση αδρεναλίνης, αν χρειαστεί.
Την εκπαίδευση της οικογένειας στην επιτυχή αντιμετώπιση μιας πιθανής μελλοντικής αλλεργικής αντίδρασης.
Συμπερασματικά,
οι αλλεργίες μπορούν να παρουσιαστούν σε οποιαδήποτε ηλικία. Έχουν
κληρονομική προδιάθεση και μπορούν να φύγουν τελείως ή να αλλάξουν
χαρακτήρα ή σύστημα εκδήλωσης όπως μεγαλώνει το παιδί. Με την κατάλληλη
θεραπεία τα συμπτώματα ελέγχονται πλήρως και τα παιδιά με αλλεργίες
μπορούν να έχουν μια απόλυτα φυσιολογική ζωή.
Allergy Awareness
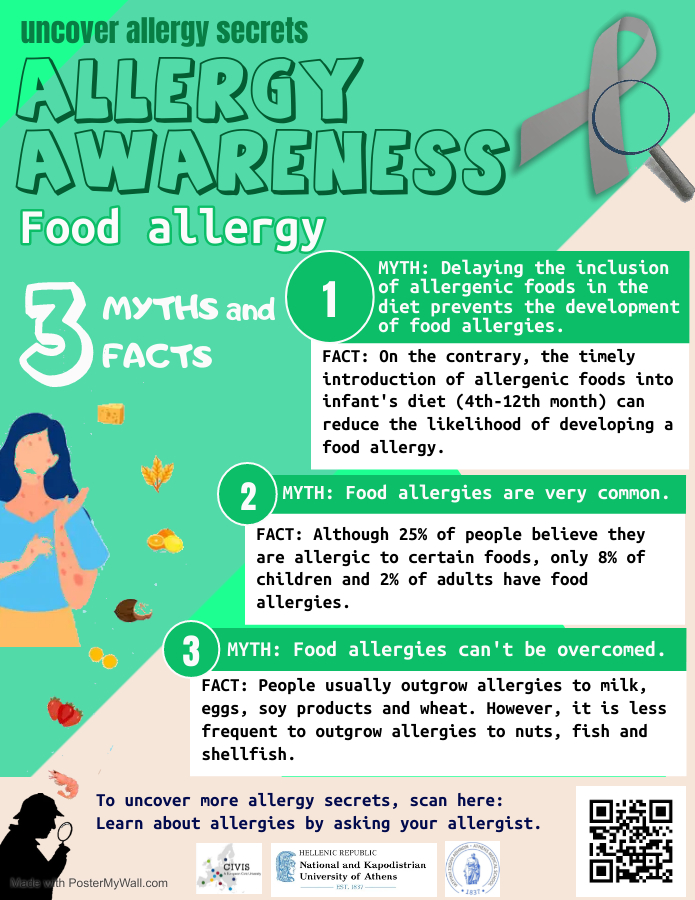
Day 1 of Allergy Awareness Week: Τροφικές Αλλεργίες
Οι αλλεργίες στα τρόφιμα συχνά χαρακτηρίζονται ως μια “αόρατη ασθένεια”, επηρεάζοντας παγκοσμίως τις ζωές πάνω από 220 εκατομμύρια ανθρώπων.
Σκοπός αυτής της καμπάνιας είναι να βοηθήσουμε την κοινότητα και ιδίως ανθρώπους με αλλεργίες και να γνωρίσουν καλύτερα τις διάφορες πτυχές της ασθένειάς τους.
Day 2 of Allergy Awareness Week: Αλλεργίες σε Ζώα και Έντομα
Οι αλλεργίες σε κατοικίδια ζώα επηρεάζουν περίπου το 20% του παγκόσμιου πληθυσμού.
Day 3 of Allergy Awareness Week: Φαρμακευτικές αλλεργίες
Οι αλλεργικές αντιδράσεις αποτελούν το 15% των πιθανών ανεπιθύμητων ενεργειών που μπορούν να προκληθούν μετά από λήψη φαρμάκων.
Ταυτόχρονα οι φαρμακευτικές αλλεργίες επηρεάζουν πάνω από το 7% του πληθυσμού.
Σκοπός αυτής της καμπάνιας είναι να βοηθήσουμε την κοινότητα και ιδίως ανθρώπους με αλλεργίες και να γνωρίσουν καλύτερα τις διάφορες πτυχές της ασθένειάς τους.
Day 4 of Allergy Awareness Week: Αλλεργική Ρινίτιδα
Η αλλεργική ρινίτιδα επηρεάζει περισσότερους από 400 εκατομμύρια ανθρώπους παγκοσμίως, αποτελώντας μια από τις πιο διαδεδομένες χρόνιες παθήσεις.
Day 5 of Allergy Awareness Week: ‘Ασθμα
Το άσθμα είναι μια από τις συχνότερες χρόνιες αναπνευστικές παθήσεις, επηρεάζοντας τόσο τις προσωπικές και όσο και τις κοινωνικές πτυχές της καθημερινότητάς των ασθενών.
H προληψη, η σωστή ενημέρωση και ο έλεγχος του άσθματος αποτελούν καθοριστικές παρεμβάσεις για την διασφάλιση μίας καλύτερης ποιότητας ζωής.
Σκοπός αυτής της καμπάνιας είναι να βοηθήσουμε την κοινότητα και ιδίως ανθρώπους με αλλεργίες και να γνωρίσουν καλύτερα τις διάφορες πτυχές της ασθένειάς τους.
Fun fact! Το άσθμα ήταν γνωστό από την αρχαιότητα, καθώς μία από τις πρώτες περιγραφές της ασθένειας ανήκουν στον Αρεταίο της Καππαδοκίας.
Day 6 of Allergy Awareness Week: Ατοπική δερματίτιδα
Η ατοπική δερματίτιδα απασχολεί περίπου το 30% του πληθυσμού με τα πρώτα συμπτώματα εμφανίζονται στα βρέφη, ήδη από τους πρώτους μήνες ζωής τους.
Σκοπός αυτής της καμπάνιας είναι να βοηθήσουμε την κοινότητα και ιδίως ανθρώπους με αλλεργίες και να γνωρίσουν καλύτερα τις διάφορες πτυχές της ασθένειάς τους.
Ας διερευνήσουμε λοιπόν μαζί κάποιους από τους συχνότερους μύθους γύρω από τις τροφικές αλλεργίες!
Από τους σημαντικότερους κινδύνους του καλοκαιριού είναι το νερό.
Μην αφήνετε τα παιδιά μόνα τους στο νερό. Οι πνιγμοί είναι η δεύτερη
συχνότερη αιτία θανάτων λόγω ατυχημάτων, στα παιδιά κάτω των 14 ετών.
Ο
πνιγμός προκαλεί τον θάνατο μέσω ασφυξίας. Η τελευταία οφείλεται ή σε
εισρόφηση του νερού από την αναπνευστική οδό ή από σπασμό του λάρυγγα
(όταν έρθει σε επαφή η επιγλωττίδα με το νερό). Η καταβύθιση σε πολύ
ψυχρό νερό μπορεί να προκαλέσει τον θάνατο μέσω υποθερμίας. Η όλη διαδικασία θέλει περίπου 5 με 10 λεπτά. (λαρυγγόσπασμος-εισρόφηση-ανεπαρκής αναπνοή και κυκλοφορία-εγκεφαλικός θάνατος).
Στα αίτια του πνιγμού περιλαμβάνονται:
• Χρήση αλκοόλ και ηρεμιστικών. • Κόπωση. • Αιφνίδια οξεία κατάσταση (π.χ έμφραγμα μυοκαρδίου , επιληψία κλπ). • Τραυματισμός της κεφαλής ή του νωτιαίου μυελού σε κατάδυση. • Δαγκώματα από υδρόβιους οργανισμούς , νόσος των δυτών κλπ. Το θύμα συνήθως είναι ωχρό ή κυανό χωρίς αναπνοή και σφυγμό.
Μπορεί να έχει αντίληψη ή να είναι σε διέγερση. Έμετος , αναπνοή με
συριγμό , ροζ αφρός από το στόμα μπορεί να παρατηρηθούν. Στην τελευταία
περίπτωση έχουμε γρήγορη και επιπόλαιη αναπνοή και ασθενικό σφυγμό.
Γενικά το θύμα είναι υποθερμικό.
Πρόληψη του πνιγμού στα παιδιά
Στις διακοπές αλλά και το σπίτι, πάρτε τα μέτρα σας και προφυλάξτε το παιδί σας από ενδεχόμενο πνιγμό.
Στην πισίνα ή τη θάλασσα
Ποτέ μην αφήνετε το παιδί σας χωρίς επίβλεψη μέσα ή κοντά σε νερό.
Μη χρησιμοποιείτε συσκευές επίπλευσης (μπρατσάκια, φουσκωτές κουλούρες κλπ) ως υποκατάστατα της επίβλεψης.
Φροντίστε
να μάθει το παιδί σας κολύμβηση όσο το δυνατόν νωρίτερα από εξειδικευμένους εκπαιδευτές. Είναι προτιμότερο να
συμμετέχετε μαζί του στα μαθήματα κολύμβησης.
Μη
θεωρήσετε ποτέ ότι το παιδί σας είναι “απρόσβλητο” από πνιγμό κι ας
ξέρει καλή κολύμβηση. Τα μικρά παιδιά (ειδικά τα κάτω των 6 ετών) πρέπει
να παρακολουθούνται στενά από ενήλικα όσο κολυμπάνε.
Διδάξετε το παιδί σας ότι δεν πρέπει ποτέ να κολυμπά μόνο του!
Μάθετε καρδιο-αναπνευστική ανάνηψη.
Στο σπίτι
Αν το παιδί σας είναι μικρό, να είστε συνεχώς μαζί του όταν κάνει μπάνιο.
Αδειάστε τη μπανιέρα μόλις τελειώσετε το μπάνιο.
Μην αφήνετε ποτέ το μεγαλύτερο παιδί να επιβλέπει το μικρότερο.
Να έχετε την πόρτα του μπάνιου κλειδωμένη, ώστε να μην μπορεί να μπει το παιδί χωρίς να το αντιληφθείτε.
Πώς μπορούμε να προλάβουμε τον πνιγμό στα παιδιά
Τα παιδιά ηλικίας
1 έως 4 ετών διατρέχουν τον υψηλότερο κίνδυνο πνιγμού και ακολουθούν οι έφηβοι.
Οι πισίνες είναι το πιο κοινό σημείο πνιγμών, αλλά είναι σημαντικό να γνωρίζουμε ότι ακόμα οι μπανιέρες, οι τουαλέτες, ακόμη και οι
κουβάδες με νερό μπορούν να αποτελέσουν κίνδυνο για βρέφη και νήπια και να
οδηγήσουν σε πνιγμό.
Ο ΠΡΑΓΜΑΤΙΚΟΣ
ΠΝΙΓΜΟΣ ΕΙΝΑΙ ΑΘΟΡΥΒΟΣ. Ίσως η πιο ισχυρή ένδειξη ότι κάποιος πνίγεται είναι
ότι δε μοιάζει να πνίγεται και αυτό γιατί:
Το άτομο που
πνίγεται
Δεν είναι σε
θέση να καλέσει βοήθεια.
Δεν μπορεί να
κουνήσει τα χέρια του έξω από το νερό ζητώντας βοήθεια.
Το σώμα
παραμένει σε κάθετη (όρθια) θέση μέσα στο νερό ενώ τα πόδια δεν κάνουν καμία
κίνηση για να το σπρώξουν προς τα πάνω.
Ο πνιγμός
συμβαίνει ΓΡΗΓΟΡΑ και ΑΘΟΡΥΒΑ, καθώς λίγα δευτερόλεπτα χαλάρωσης της προσοχής
των γονιών είναι αρκετά για να πνιγεί ένα παιδί. Τα βρέφη και τα πολύ μικρά
παιδιά είναι περισσότερο ευάλωτα σε πνιγμό από ελάχιστη ποσότητα νερού καθώς
δεν έχουν αναπτύξει πλήρως τους σωματικούς μηχανισμούς αντίδρασης σε περίπτωση
κατάποσης θαλασσινού νερού.
Ο πνιγμός στα
παιδιά είναι αθόρυβος, γιατί το παιδί δεν έχει προηγούμενη εμπειρία ασφυξίας
και δε θα καλέσει σε βοήθεια και μπορεί να συμβεί, χωρίς φωνές για βοήθεια,
χωρίς χέρια που ανεμίζουν πάνω από την επιφάνεια του νερού.
ΝΚ
Πώς μπορούμε να προλάβουμε τον πνιγμό στα παιδιά
1. Δεν αφήνουμε ούτε δευτερόλεπτο το παιδί από τα μάτια μας
2. Όταν επιβλέπουμε παιδιά που κολυμπούν δεν πίνουμε καφέ, αλκοόλ, δεν καπνίζουμε, δεν μιλάμε στο τηλέφωνο, δεν παίζουμε χαρτιά.
3. Δεν εμπιστευόμαστε ούτε τα παιδιά που ξέρουν κολύμπι.
4. Δεν εμπιστευόμαστε την παρουσία ναυαγοσώστη.
5. Δεν αναθέτουμε το καθήκον της επίβλεψης σε μεγαλύτερα παιδιά ή σε υπερήλικα άτομα.
6. Αν χρειαστεί να απομακρυνθούμε έστω και για λίγο παίρνουμε και το παιδί μαζί μας.
7. Δεν τα αφήνετε να κάνουν βουτιές σε άγνωστα νερά, σε ρηχά νερά, σε νερά με βράχια.
8. Μάθετε το παιδί να κολυμπάει από την πιο μικρή δυνατή ηλικία..
Δρ.Νίκος Κονναρής -Παιδίατρος
Οδηγίες για τους κολυμβητές
Να κολυμπάτε πάντα με παρέα. Ποτέ μόνοι και ποτέ σε ερημιά.
Περιμένετε να περάσουν 4 ώρες από το φαγητό για να κολυμπήσετε.
Τα οινοπνευματώδη ποτά και η κολύμβηση είναι επικίνδυνος συνδυασμός.
Μην κολυμπάτε όταν οι καιρικές συνθήκες είναι κακές (ειδικά όταν βρέχει) και σε θάλασσα με μεγάλα κύματα ή ισχυρά ρεύματα.
Μην κολυμπάτε κοντά στα βράχια
Μην κάνετε βουτιές σε άγνωστα ή θολά νερά ή σε περιοχές με βράχια και πέτρες.
Μην περνάτε τις σημαδούρες που ορίζουν τη ζώνη κολύμβησης στις οργανωμένες παραλίες.
Μην κολυμπάτε στα ανοιχτά ιδίως σε πολυσύχναστες παραλίες όπου περνάνε βάρκες ή ταχύπλοα.
Αν
κάνετε υποβρύχιο ψάρεμα ή καταδύσεις, να χρησιμοποιείτε πάντα τον
εξοπλισμό ασφαλείας (σημαδούρα με σημαιάκι) και να είστε οπωσδήποτε μαζί
με έμπειρο ενήλικα.
Μη σπρώχνετε και μη βυθίζετε τους άλλους στο νερό.
Βγείτε από το νερό αν δεν νιώθετε καλά, αν φοβάστε ή αν κρυώνετε.
Καλέστε για βοήθεια αν νιώσετε κίνδυνο.
Αν
κάποιος κινδυνεύει στο νερό βρείτε ένα αντικείμενο που επιπλέει και
ρίξτε το κοντά του για να πιαστεί. Παράλληλα φωνάξτε για βοήθεια.
Προσοχή:
μην πλησιάσετε το θύμα γιατί μπορεί να κινδυνέψετε και εσείς αν πιαστεί
πάνω σας. Ο αλτρουισμός και η αυτοθυσία δεν ωφελεί αν δεν κατευθύνεται
από τη λογική.
Έχετε μαζί σας, στην παραλία, στο αυτοκίνητο, στη βάρκα, το κουτί πρώτων βοηθειών.
Μάθετε καρδιο-αναπνευστική ανάνηψη και να θυμάστε το τηλέφωνο των πρώτων βοηθειών(112).
Children and headaches Red flags, triggers, and rescue treatments
(Contemporary PEDS Journal, Vol 38 No 5)-Πονοκέφαλος στα παιδιά
Headaches
are 1 of the top 5 health problems of childhood.Because 58.4% of
children and adolescents aged 1 month or older will develop will develop
headaches at some point, general pediatric practitioners may have many
opportunities to evaluate and treat patients with headaches
Πονοκέφαλος στα παιδιά
...Η
κεφαλαλγία αποτελεί συχνό σύμπτωμα στα παιδιά και μάλιστα αποτελεί τη
δεύτερη σε συχνότητα εντόπιση πόνου, για την οποία απευθύνονται τα
παιδιά στον παιδίατρο. Αντιπροσωπεύει το 2% του συνόλου των επισκέψεων
στον παιδίατρο.
Συνήθως,
δεν είναι κάτι σοβαρό. Συναντάται σε όλες τις ηλικίες, αλλά είναι σαφώς
συχνότερη στους εφήβους και, κυρίως, στα κορίτσια.
Η
κεφαλαλγία εκφράζεται ως πόνος στην επιφάνεια της κεφαλής και
προκαλείται από ερεθίσματα, τα οποία προέρχονται από ενδοκρανιακά, αλλά
και εξωκρανιακά αίτια.
Ο
εγκέφαλος είναι πρακτικά αναίσθητος στον πόνο, άρα κατά κανόνα η
κεφαλαλγία δεν προκαλείται από βλάβες του ίδιου του εγκεφάλου. Αντίθετα,
ερέθισμα, που αφορά στα αγγεία της σκληρής μήνιγγας, μπορεί να
προκαλέσει κεφαλαλγία.
Οι
κεφαλαλγίες χωρίζονται σε πρωτοπαθείς και δευτεροπαθείς. Οι πρωτοπαθείς
περιλαμβάνουν καταστάσεις αδιευκρίνιστης αιτιολογίας, που δεν απειλούν
τη ζωή του ασθενούς, αλλά είναι ιδιαίτερα ενοχλητικές. Αντίθετα, οι
δευτεροπαθείς οφείλονται σε ποικίλα αίτια και, συχνά, είναι απειλητικές
για τη ζωή του ασθενούς.
Οι πονοκέφαλοι στα παιδιά είναι συχνοί και συνήθως δεν
είναι σοβαροί. Όπως οι ενήλικες, τα παιδιά μπορεί να αναπτύξουν διαφορετικούς
τύπους πονοκεφάλων, συμπεριλαμβανομένων των ημικρανιών ή των πονοκεφάλων (τασης)
που σχετίζονται με το στρες. Τα παιδιά μπορεί επίσης να έχουν χρόνιους
καθημερινούς πονοκεφάλους.
Σε ορισμένες περιπτώσεις, οι πονοκέφαλοι στα παιδιά
προκαλούνται από μόλυνση, υψηλά επίπεδα στρες ή άγχους ή τραύμα στο κεφάλι. Είναι σημαντικό να δίνετε
προσοχή στα συμπτώματα πονοκεφάλου του παιδιού σας και να συμβουλευτείτε έναν
γιατρό εάν ο πονοκέφαλος επιδεινώνεται ή εμφανίζεται συχνά.
Οι πονοκέφαλοι στα παιδιά συνήθως μπορούν να
αντιμετωπιστούν με παυσίπονα χωρίς ιατρική συνταγή (OTC) και υγιεινές
συνήθειες, όπως ένα τακτικό πρόγραμμα ύπνου και φαγητού.
Οι περισσότεροι πονοκέφαλοι δεν είναι σοβαροί, αλλά
αναζητήστε άμεση ιατρική φροντίδα εάν οι πονοκέφαλοι του παιδιού σας:
Ξυπνούν το
παιδί σας από τον ύπνο
Επιδεινώνονταιται ή
γίνονται πιο συχνοί
Προκαλούν αλλαγές στην
προσωπικότητα του παιδιού σας
Αν εμφανιστούν μετά απο
έναν τραυματισμό, όπως ένα χτύπημα στο κεφάλι
Συνοδεύονται απο επίμονους εμετούς ή οπτικέςδιαταραχές
Συνοδεύονται
από πυρετό και πόνο στον αυχένα ή δυσκαμψία
Many
conditions can present initially with headache, so it is important to
have a list of “red flag” risk factors, symptoms, and exam findings to
keep in mind during the initial assessment. Red flag risk factors would
include a patient aged younger than 6 years, history of neurocutaneous
syndrome, systemic illness, immunodeficiency, known malignancy, or
hypercoagulability.2
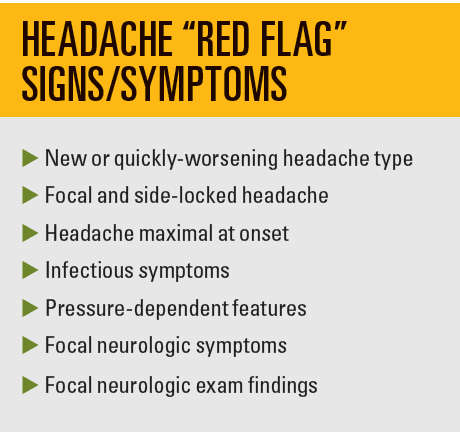
Red
flag symptoms include new (< 1 month) or quickly worsening headache
type, focal and sidelocked headache, headache maximal at onset
(thunderclap headache), infectious symptoms (eg, fever, meningismus,
sinus or ear pain), or pressure-dependent features (eg, positional
headache), headache worse in the middle of the night or first thing in
the morning, headaches triggered by cough or Valsalva maneuvers,
vomiting that is persistent and increasing in frequency. Focal
neurologic symptoms or exam findings (eg, seizures, vision changes,
papilledema, ataxia) also require urgent evaluation. Etiologies that
cannot be missed include mass lesions, infections (eg,
meningitis/encephalitis, brain abscess), and vascular etiologies (eg,
stroke, hemorrhage, aneurysm, arteriovenous malformation, cerebral
venous sinus thrombosis). Any of these symptoms or exam findings should
prompt urgent consideration of brain imaging and/or lumbar puncture.
Less than 1% of brain abnormalities in patients present with chronic
headache as the only symptom.3
Primary versus secondary headaches
Once
urgent headache etiologies are no longer of concern, the next objective
is to distinguish between primary and secondary headaches. Unlike
secondary headaches, primary headaches, such as migraine and
tension-type headaches, are not a symptom of an underlying issue.
Whereas a child may develop migraine-type headaches due to obstructive
sleep apnea, the diagnosis of primary headache is only made after
excluding the possibility of a secondary headache disorder. Depending on
the history and physical exam, as well as diagnostic testing when
needed (eg, screening blood tests or sleep study), the differentiation
between primary and secondary headache can be made.
Primary headaches
The
diagnosis of primary headache is made primarily through identifying
classic characteristics of the headache, as there are no confirmatory
diagnostic tests. The International Headache Society has created an
International Classification of Headache Disorders to aid clinicians and
investigators.4,5
The diagnosis of episodic childhood
migraine is adapted from adult migraine. It is defined as an episodic
headache with 5 or more attacks that last 2 to 72 hours. It must have 2
or more of the following: unilateral or bilateral location, pulsating
quality, moderate to severe pain, or aggravation by routine physical
activity. It must also have 1 or more of the following: nausea or
vomiting, and photophobia and phonophobia. For childhood migraine,
experts argue that headaches are often shorter, lasting 30 minutes or
more, and often fitting 1 or more of each category.6
Premonitory signs also are different in childhood migraine than in adult
migraine. They are most commonly fatigue, mood changes, neck stiffness,
cranial autonomic symptoms, and cutaneous allodynia, rather than visual
disturbance or dizziness.7
Diagnosing episodic
childhood tension-type headache requires 10 or more episodes lasting
from 30 minutes to 7 days. It must have 2 or more of the following:
bilateral location, pressing or tightening quality (nonpulsating), mild
or moderate intensity, and it cannot be aggravated by routine physical
activity. There cannot be nausea or vomiting, and no more than 1 of
photophobia or phonophobia.
Children and adolescents may present
with both migraine and tension-type headaches, making it difficult to
have separate treatment trials. In fact, it is unclear whether they are
actual separate biological entities.8 Most treatments are
geared toward migraine management, but the overall approach for both
should be 3-pronged, addressing lifestyle modifications, a rescue plan,
and a preventative plan.
Headache treatment: Lifestyle modification
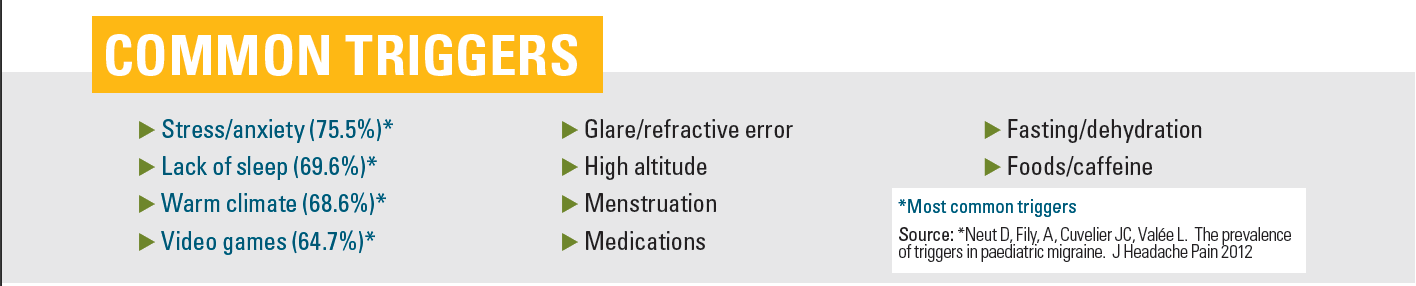
The most common triggers for childhood headache include stress/anxiety, lack of sleep, warm climate, and video games.9
Other triggers include glare, eye strain, high altitude, menstruation,
medications, fasting, dehydration, certain foods (eg, simple sugars,
smoked meats, chocolate), caffeine use, and lack of exercise.
The
first step in headache treatment is to better characterize the headaches
and triggers by keeping a headache diary documenting possible triggers,
time of day, days per month, headache intensity, and response to
treatment. The number and/or intensity of headaches over time influences
what types of treatment are needed. For example, episodic headaches
(less than 2 times a week) can be treated with rescue medications alone,
whereas headaches more frequent than that will require preventative
treatment as well as rescue medications.
The general categories
for lifestyle modifications are water and food intake, sleep regulation,
daily exercise, and stress reduction.
Headache treatment rescue plan
Tip: Tell patients and their caregivers that the rescue plan should be implemented right at the beginning of the headache.
Because
of the nature of the headache/pain cycle with amplification over time,
the longer it takes to treat, the harder it is to break the cycle.
Taking rescue measures early and taking the full dose of the abortive
medication are more effective than waiting and then giving a half dose
followed by another half dose.
Caregivers should be cautioned that
these medications are only meant for rescue. Taking them more than 2 or
3 times a week over a month-long period can lead to medication overuse
headache syndrome.
Nausea and vomiting are most common in younger children as part of the headache syndrome,10 and
antiemetics can be used in conjunction with headache medications. As
patients who are nauseated may not tolerate swallowing pills, many
headache medications come in oral-dissolving or intranasal formulations.
The
first line for abortive headache treatments includes acetaminophen,
ibuprofen, and other nonsteroidal anti-inflammatory drugs. Randomized
trials for pharmacologic rescue treatments efficacy show acetaminophen
at 54% and ibuprofen at 68.76%.11
Triptan
medications, the second line for rescue headache treatments, were
designed specifically to abort migraine headaches. Because they have
selective activity on atypical 5HT1B and 5HT1D receptors, their
mechanisms of action include cranial vasoconstriction, peripheral
trigeminal inhibition, and inhibition of transmission via the trigeminal
cervical complex. They are typically well tolerated. Common adverse
effects include paresthesia, sleepiness, dizziness, and tightness in
chest or throat. They should not be used more than 2 times a week and
should be avoided in patients with cardiovascular disease, who are
pregnant, or who have complicated migraines. Rizatriptan (efficacy
73-74%) is the only treatment approved for patients aged 6 to 12 years.
Sumatriptan nasal spray (64-86%), combination sumatriptan/naproxen,
almotriptan (72-73%), and zolmitriptan nasal spray (62%) are approved in
patients aged 12 to 17 years.11
Further pharmacologic
rescue treatments typically have to be administered intravenously in the
emergency department setting. Of the dopamine antagonists,
prochlorperazine (Compazine) IV is the most effective abortive in
randomized trials at 84.8% pain relief, followed by metoclopramide
(Reglan) and promethazine (Phenergan).12,13
Headache treatment-preventive plan
Whereas
patients with episodic headache can often be treated with lifestyle
changes and rescue medications alone, others with chronic headaches
(> 15 days a month) and severe headaches will benefit from a
preventive plan that aims to decrease both headache severity and
frequency.
Tip: it is important to distinguish rescue from
preventive treatment, so patients do not stop taking preventive
treatments within few days when it “doesn’t work.”
Patients should
understand that preventive treatment has to start at a low dose to
minimize adverse effects and build up slowly. Within 6 to 8 weeks of
taking it constantly, the goal would be a decrease in headache frequency
and intensity by at least 50%.
For many years, the use of
pharmacologic preventive medications in childhood headache was based on
adult studies. A seminal paper published in The New England Journal of Medicine
in 2018 based on the CHAMP trial (NCT01581281) compared children with
episodic migraine in 3 prospective randomized groups taking placebo,
topiramate 2 mg/kg, or amitriptyline 1 mg/kg.14 The trial was
stopped early because the placebo group did as well as the other 2
groups with fewer adverse effects. It was noted that patients had an
average of 11 days per month of headache (suggesting more of an episodic
than chronic headache picture) and that the placebo group received
appropriate lifestyle management and rescue plan counseling. This
underscores the efficacy of lifestyle and rescue management independent
of pharmacologic preventive therapy.
Following this study, many
practitioners chose to offer nutraceuticals for headache prevention
before going straight to pharmacologic treatments. Nutraceuticals
include vitamins, minerals, herbal supplements, and dietary supplements.
Magnesium, riboflavin (vitamin B2), coenzyme Q10, and vitamin D3 all have demonstrated efficacy in some pediatric trials for headache prevention,15-18
although there are limited studies with a placebo group. Importantly,
the adverse effect profile for nutraceuticals is better than for
pharmacologic agents.
If headaches continue to be troublesome
despite lifestyle management, good rescue therapy, and a sustained trial
of nutraceuticals, it is reasonable to consider pharmacologic
preventatives. Cyproheptadine (Periactin), an antihistamine, has no
clinical trial data but has probably been used the longest for pediatric
headache prevention. Although it is well-tolerated in younger children,
patients 8 years of age and older typically experience too much
sedation for it to be acceptable. Topiramate, an epileptic medication,
received FDA approval in 2014 for the prevention of headaches in
adolescents aged 12 to 17 years. Potential common adverse effects
include cognitive slowing, paresthesias, appetite suppression, and renal
stones. Amitriptyline, an antidepressant, can be helpful for patients
with migraines who also have insomnia and/or depression. Besides
somnolence, it can cause appetite increase, tachycardia, and dry mouth.
Propranolol, a β-blocker, has 1 randomized control trial from 1974
showing efficacy, but subsequent studies have been negative. Possible
adverse effects include exercise intolerance, depression, and
light-headedness.
Finally, there are many other nonpharmacologic
interventions that have been shown to be helpful in mitigating childhood
headache and may have a synergistic effect with preventive medications.
Cognitive behavioral therapy (CBT) in combination with amitriptyline
was more beneficial than CBT alone for a group of adolescents.19
There is some convincing evidence for biofeedback (teaching patients to
regulate physical responses to stress) in the prevention of pediatric
migraine, sometimes in combination with relaxation therapy. At Stanford
Children’s Health, occupational therapists and pediatric pain
psychologists are trained in multiple modalities such at CBT,
biofeedback, and relaxation therapy. If there is a history of
neck/shoulder pain or tenderness to palpation of the scalp, neck, or
shoulders, a physical therapist can help strengthen and realign a
patient’s posture to prevent cervicogenic headache. There is 1 positive
study on acupuncture for pediatric headache,20 and many adult
studies demonstrate efficacy in chronic pain and headache. It is
important to explain to the patient that acupuncture needles are much
thinner and less painful than typical needles; children who have had
acupuncture before seem to prefer this method.
When to refer to a neurologist
Instances
in which consultation with a neurologist could be helpful would include
headaches that are severe, prolonged, or intractable. Neurology
consultation would be indicated for patients with a complicated aura
(eg, hemiplegic migraine or migraine with brainstem symptoms such as
dysarthria, vertigo, tinnitus, or diplopia). Referral is advised when a
pediatric practitioner is reconsidering the diagnosis of primary
headaches and would like guidance on workup for secondary headaches.
Finally, a practitioner may feel comfortable implementing first- or
second-line therapies but will seek help with less conventional
treatments, such as the new class of anti-cGRP monoclonal antibodies.
These have not yet been approved in children but are increasingly being
prescribed off label for adolescents with intractable migraines. The
American Headache Society Section on Pediatric-Adolescent Headache
offers guidelines for administering these new treatments.21
Several neuromodulatory devices have been developed for the headache
population, with 2 approved by the FDA for adolescents, but the studies
have very small sizes (9-45 patients) and the cost for renting these
devices is often prohibitive.
Childhood headache can be dangerous,
debilitating, or both. After excluding dangerous causes, it is
important to provide the patient and caregiver with a plan for headache
management that includes education on lifestyle management, rescue plan,
and preventive measures. During the current pandemic, screen time and
eye strain have become more significant triggers, whereas, conversely,
being able to sleep in later on school days appears to be beneficial for
teenagers.22,23 The more that children and their caregivers
are empowered to understand and manage childhood headaches, the better
for all involved.
SOURCES: CONTEMPORARY PEDIATRICS, MAYO CLINIC,AAP
References
Abu-Arafeh
I, Razek S, Sivaraman B, Graham C. Prevalence of headache and migraine
in children and adolescents: a systematic review of population-based
studies. Dev Med Child Neurol. 2010;52(12):1088-1097. doi:10.1111/j.1469-8749.2010.03793
Parisi P, Papetti L, Spalice A, Nicita F, Ursitti F, Villa MP. Tension-type headache in paediatric age. Acta Paediatr. 2011;100(4):491-495. doi:10.1111/j.1651-2227.2010.02115.x
Abu-Arafeh I, McLeod S. Serious neurologic disorders in children with chronic headache. Arch Dis Child. 2005;90(9):937-940. doi:10.1136/adc.2004.067256
Headache Classification
Committee of the International Headache Society (IHS) The International
Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1-211. doi:10.1177/0333102417738202
Özge
A, Faedda N, Abu-Arafeh I, et al. Experts’ opinion about the
primary headache diagnostic criteria of the ICHD-3rd edition beta in
children and adolescents. J Headache Pain. 2017;18(1):109. doi:10.1186/s10194-017-0818-y
Karsan
N, Prabhakar P, Goadsby PJ. Characterising the premonitory stage of
migraine in children: a clinic-based study of 100 patients in a
specialist headache service. J Headache Pain. 2016;17(1):94.doi:10.1186/s10194-016-0689-7
Monteith TS, Sprenger T. Tension type headache in adolescence and childhood: where are we now?Curr Pain Headache Rep. 2010;14(6):424-430. doi:10.1007/s11916-010-0149-z
Neut D et al. The prevalence of triggers in paediatric migraine: a questionnaire study in 102 children and adolescents. J Headache Pain. 2012;13(1):61-65. doi:10.1007/s10194-011-0397-2
Wilcox
SL, Ludwick AM, Lebel A, Borsook D. Age- and sex-related differences in
the presentation of paediatric migraine: A retrospective cohort study. Cephalalgia. 2018; 38(6):1107-1118. doi:10.1177/0333102417722570
Gelfand A, Goadsby PJ. Treatment of pediatric migraine in the emergency room. Pediatr Neurol. 2012;47(4):233-241. doi:10.1016/j.pediatrneurol.2012.06.001
Sheridan
DC, Laurie A, Pacheco S, et al. Relative effectiveness of dopamine
antagonists for pediatric migraine in the emergency department. Pediatr Emer Care. 2018;34(3):165-168. doi:10.1097/PEC.0000000000000718
Bachur RG, Monuteaux MC, Neuman MI. A comparison of acute treatment regimens for migraine in the emergency department. Pediatrics. 2015;135(2):232-238. doi:10.1542/peds.2014-2432
Powers SW, Coffey CS, Chamberlin LA, et al. Trial of amitriptyline, topiramate, and placebo for pediatric migraine. N Engl J Med. 2017;376(2):115-124. doi:10.1056/NEJMoa1610384
Wang
F, Van Den Eeden SK, Ackerson LM, Salk SE, Reince RH, Elin RJ. Oral
magnesium oxide prophylaxis of frequent migrainous headache in children:
a randomized, double-blind, placebo-controlled trial. Headache. 2003;43(6):601-610. doi:10.1046/j.1526-4610.2003.03102.x
Das R, Qubty W. Retrospective observational study on riboflavin prophylaxis in child and adolescent migraine. Pediatric Neurology. 2021;114:5-8. doi:10.1016/j.pediatrneurol.2020.09.009
Slater
SK, Nelson TD, Kabbouche MA, et al. A randomized, double-blinded,
placebo-controlled, crossover, add-on study of coenzyme Q10 in the
prevention of pediatric and adolescent migraine. Cephalalgia. 2011;31(8):897-905. doi:10.1177/0333102411406755
Fallah
R, Yazd SS, Sohrevardi SM. Efficacy of topiramate alone and topiramate
plus vitamin D3 in the prophylaxis of pediatric migraine: a randomized
clinical trial. Iran J Child Neurol. 2020;14(4):77-86. doi:10.22037/ijcn.v15i1.18017
Powers
SW, Kashikar-Zuck SM, Allen JR, et al. Cognitive behavioral therapy
plus amitriptyline for chronic migraine in children and adolescents: a
randomized clinical trial. JAMA. 2013;310(24):2622-2630. doi:10.1001/jama.2013.282533
Pintov S, Lahat E, Alstein M, Vogel Z, Barg J. Acupuncture and the opioid system: implications in management of migraine. Pediatr Neurol. 1997;17(2):129-133. doi:10.1016/s0887-8994(97)00086-6
Szperka
CL, VanderPluym J, Orr SL, et al. Recommendations on the use of
anti-CGRP monoclonal antibodies in children and adolescents. Headache. 2018;58(10):1658-1669. doi:10.1111/head.13414
Gelfand AA, Pavitt S, Ross AC, et al. Later high school start time is associated with lower migraine frequency in adolescents. Headache. 2021;61(2):343-350.doi:10.1111/head.14016




















{kind=link}